



DDI has been testing a protocol to reduce dose to children for orthodontic applications, and we have asked Arun a few questions about this to understand the capabilities of the I-CAT.
We tested this using the 13cm height with a 10 second scan mode. Then we imported the data into Dolphin 3D and created the typical ortho views plus added views like TM joint, airway and 3D renderings. When I asked Arun how much time the patient was being exposed to the pulsed 10 second scan he said “Less than 1.75 seconds” Arun further stated that “Dose could be lowered further, perhaps dramatically, we (ISI) intend to launch a project to investigate this soon”.
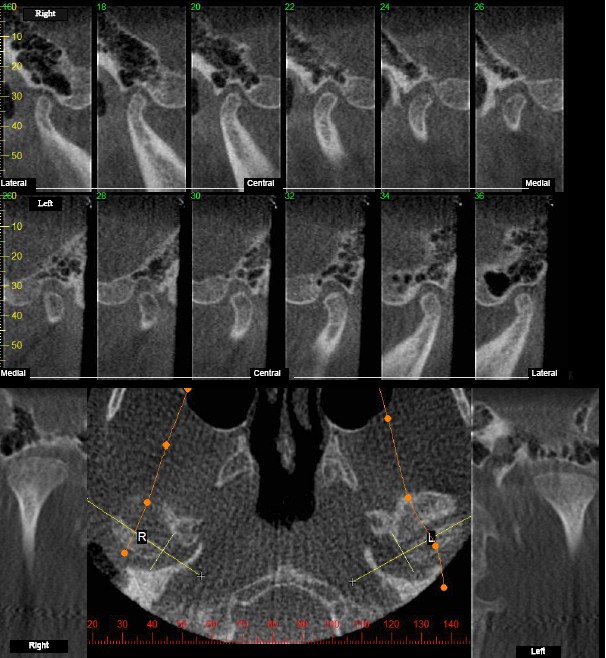
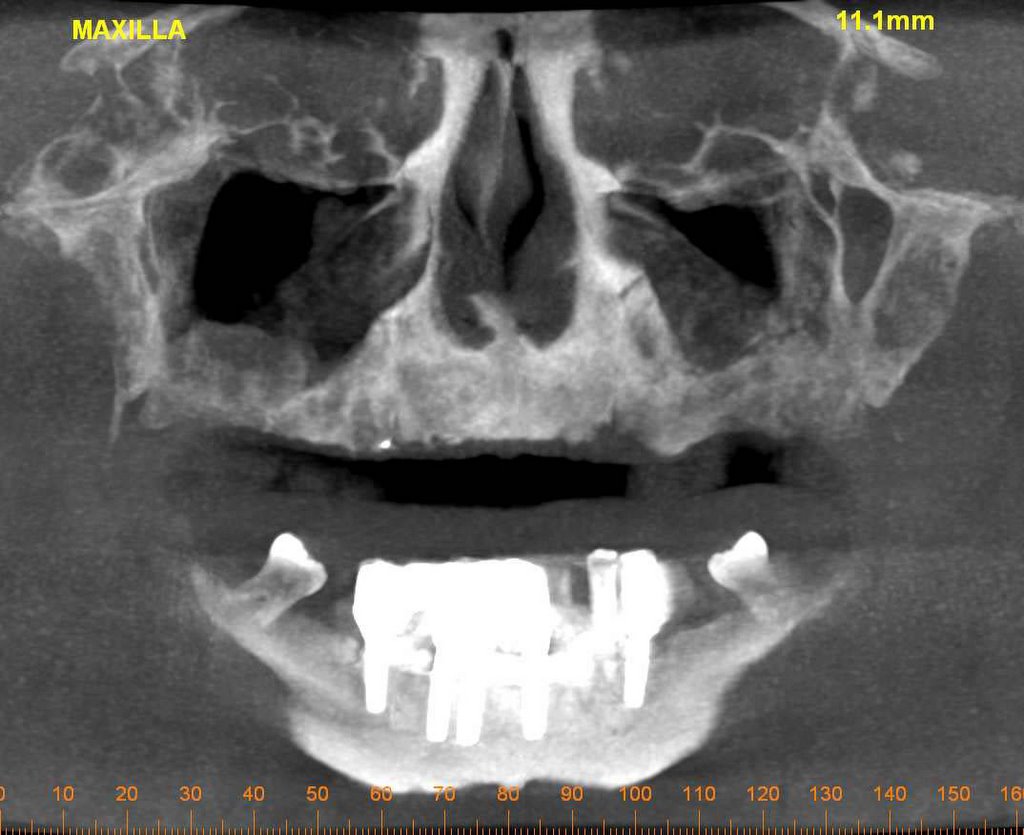
We tested this theory by doing a scan on a orthodontist that was asking the question about mid treatment scans. His thoughts were that we may do a higher resolution scan in the beginning ortho to rule out any abnormalities, and if the case was a “standard” case, then at mid-treatment, we could consider doing a low resolution scan.
The images attached is of the Orthodontist, and the images should be of better quality if we use a child.








{kind=link}